

TL;DR
There is no FDA-approved TB-500 dosing protocol. Current protocols come from animal research, practitioner experience, and real-world use.
The most common protocol uses a loading phase of 2 to 2.5 mg twice weekly for 4 to 6 weeks, followed by a maintenance dose of 2 mg once weekly.
A typical TB-500 cycle lasts 8 to 12 weeks, followed by a 4-week break because long-term continuous use has not been studied.
TB-500 is generally injected subcutaneously, and injecting near the injury is not considered necessary because it is thought to work systemically.
Store reconstituted TB-500 in the refrigerator at 2 to 8°C (36 to 46°F) and always buy from vendors that provide an independent third-party Certificate of Analysis (COA).
Let's establish one thing at the beginning. There's no FDA-approved dosing chart for TB-500, and every protocol you will find online comes from animal research and what real-world users have found over the years.
That's not a knock on it; we are just being transparent. We care about your choices, and providing verified peptide information is what separates ONPEPS from others.
The standard TB-500 protocol runs in two phases: a loading phase to get repair processes moving, then a maintenance phase to keep things going while tissue finishes healing.
Why Does the TB-500 Protocol Have Two Phases?
Research has shown that tissue repair needs a push of peptide availability at the start to drive cell migration and new blood vessel growth at the injury site. This gets the ball rolling, and then a lower weekly dose keeps it sustained. That's why TB-500 has a loading phase and a maintenance phase.
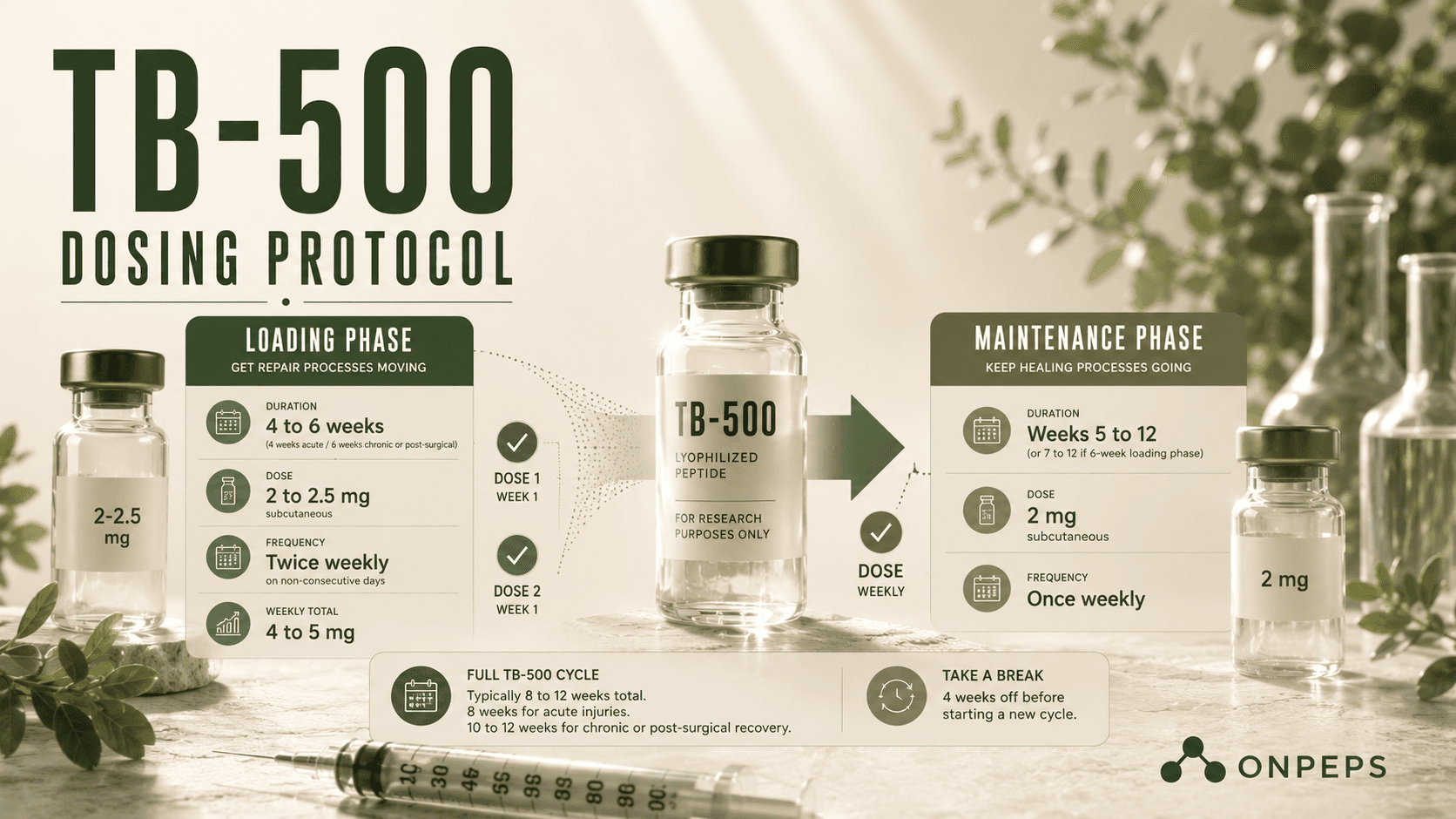
TB-500 Loading Phase Dose
How long: 4 weeks for acute injuries, 6 weeks for chronic or post-surgical cases
Dose: 2 to 2.5 mg subcutaneous, twice a week, on non-consecutive days (think Monday/Thursday or Tuesday/Friday)
Weekly total: 4 to 5 mg
Parameter | Recommendation |
Duration | 4 weeks (acute injuries), 6 weeks (chronic or post-surgical recovery) |
Dose | 2 to 2.5 mg, twice weekly |
Weekly Total | 4 to 5 mg |
Injection Route | Subcutaneous |
Injection Schedule | Non-consecutive days (e.g., Monday/Thursday or Tuesday/Friday) |
Some people in the peptide community push higher, using 4 to 5 mg per injection, twice weekly (8 to 10 mg per week), for severe or long-standing injuries.
That's on the aggressive end, and there's no human dose-finding data backing that specific number for the TB-500 fragment. That is worth knowing before you go there. There is a benefit to spacing doses on non-consecutive days. It keeps peptide levels steady without cramming injections too close together.
TB-500 Maintenance Phase Dose
How long: Weeks 5 to 12 (or weeks 7 to 12 if you ran the 6-week loading phase)
Dose: 2 mg subcutaneous, once a week
Some people taper to 2 mg every two weeks toward the end of the cycle, especially for acute injuries that are clearly improving by week 6.
Parameter | Protocol |
Duration | 4 weeks (acute injuries) or 6 weeks (chronic or post-surgical recovery) |
Dose | 2 to 2.5 mg |
Frequency | Twice weekly |
Weekly Total | 4 to 5 mg |
Route | Subcutaneous injection |
Injection Schedule | Non-consecutive days (e.g. Monday/Thursday or Tuesday/Friday) |
How Long Should You Run a Full TB-500 Cycle?
A full TB-500 cycle is typically 8 to 12 weeks. Acute sports injuries usually wrap up around 8 weeks. Chronic tendon issues or post-surgical recovery tend to run the full 10 to 12 weeks.
After that, take a 4-week break before starting again. Running TB-500 continuously, back to back with no break, isn't something the data supports one way or the other, so the break is the safer default.
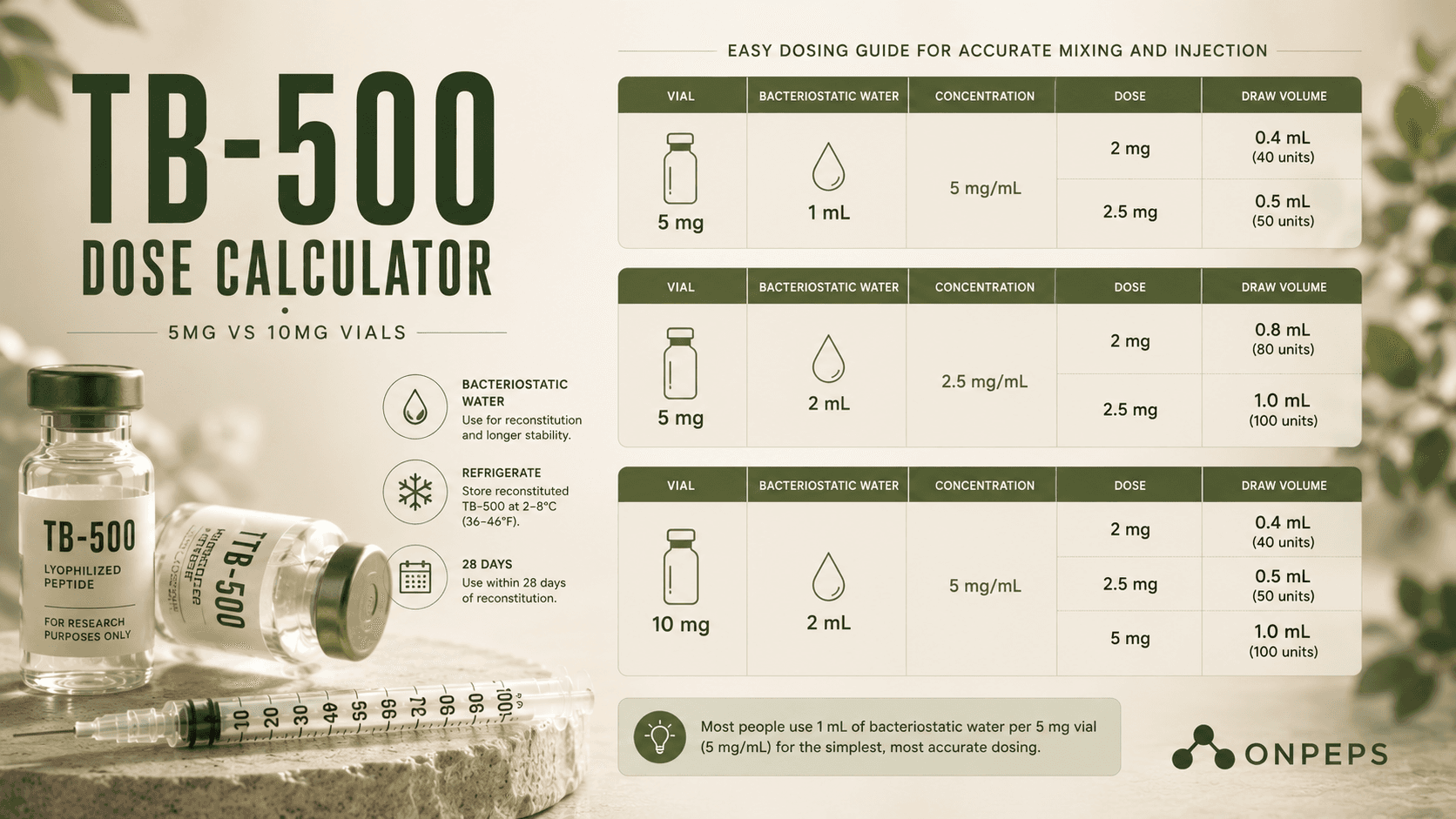
TB-500 Dose Calculator: 5mg vs 10mg Vials
This trips people up more than anything else, so here's the breakdown.
5 mg vial + 1 mL bacteriostatic water = 5 mg/mL
2 mg dose = 0.4 mL (40 units on a standard insulin syringe)
2.5 mg dose = 0.5 mL (50 units)
5 mg vial + 2 mL bacteriostatic water = 2.5 mg/mL
2 mg dose = 0.8 mL (80 units)
2.5 mg dose = 1 mL (100 units, full syringe)
10 mg vial + 2 mL bacteriostatic water = 5 mg/mL
2 mg dose = 0.4 mL (40 units)
2.5 mg dose = 0.5 mL (50 units)
5 mg dose = 1.0 mL (100 units)
Most people stick with the 1 mL per 5 mg ratio because the numbers come out clean and easy to draw.
Vial | Bacteriostatic Water | Concentration | Dose | Draw Volume |
|---|---|---|---|---|
5 mg | 1 mL | 5 mg/mL | 2 mg | 0.4 mL (40 units) |
5 mg | 1 mL | 5 mg/mL | 2.5 mg | 0.5 mL (50 units) |
5 mg | 2 mL | 2.5 mg/mL | 2 mg | 0.8 mL (80 units) |
5 mg | 2 mL | 2.5 mg/mL | 2.5 mg | 1.0 mL (100 units) |
10 mg | 2 mL | 5 mg/mL | 2 mg | 0.4 mL (40 units) |
10 mg | 2 mL | 5 mg/mL | 2.5 mg | 0.5 mL (50 units) |
10 mg | 2 mL | 5 mg/mL | 5 mg | 1.0 mL (100 units) |
How Do You Use or Inject TB-500?
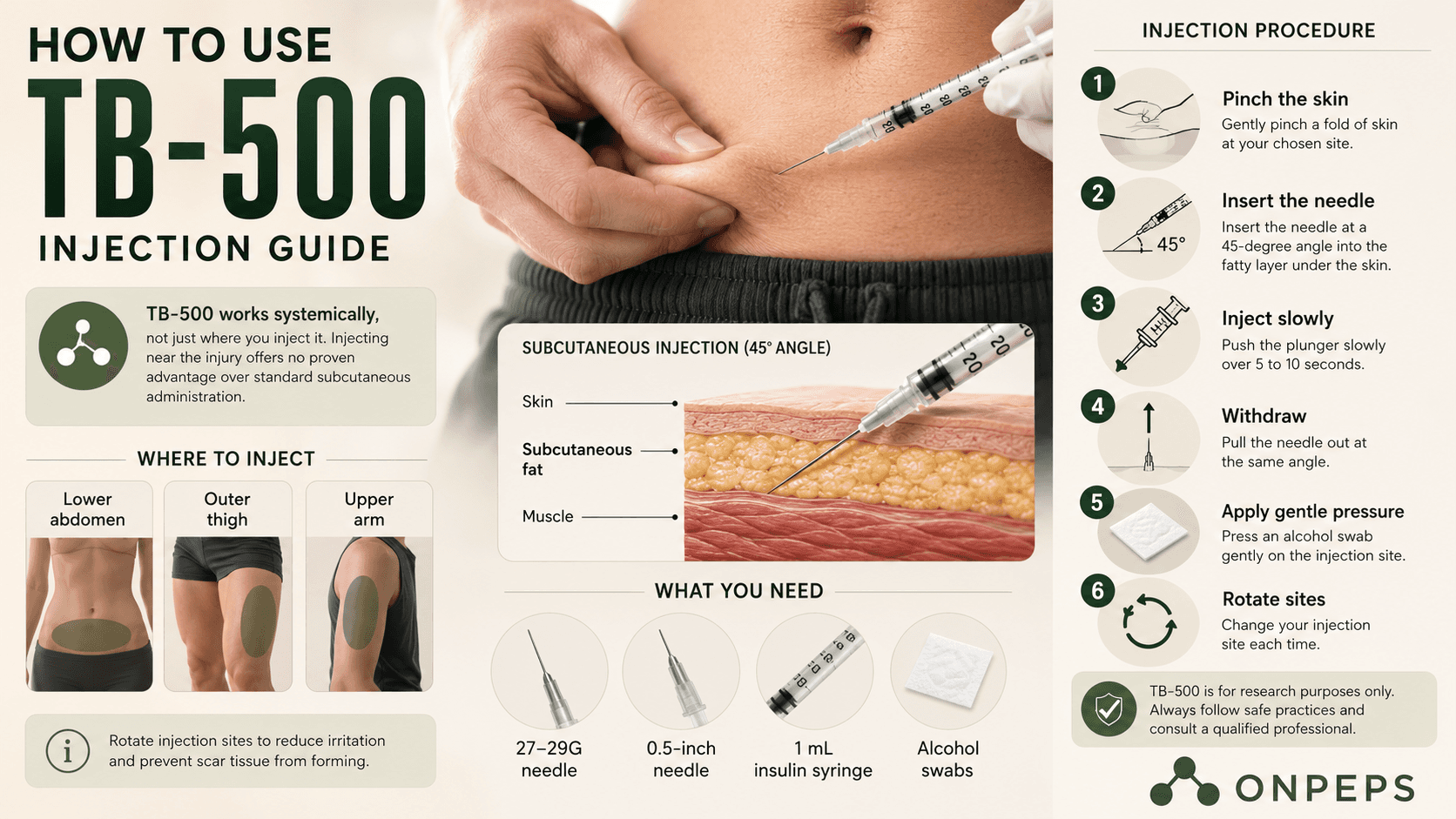
TB-500 is used subcutaneously (under the skin), and a key thing to remember is that TB-500 works throughout your body, not just where you inject it. If you remember from our BPC-157 dosage article (if you haven't read it yet, here's your chance to demystify BPC-157), it works best close to the injury. But TB-500 is circulates and reaches injury sites regardless of where you inject the peptide.
So injecting near the injury doesn't give you any extra benefit, and going intramuscular instead of subcutaneous just adds discomfort for no real upside.
Injection procedure:
What you need: 27 to 29 gauge, 0.5-inch needle, 1 mL insulin syringe, alcohol swabs
Pinch a fold of skin. Lower abdomen, outer thigh, or upper arm all work fine.
Insert the needle at a 45-degree angle into the fatty layer under the skin.
Push the plunger slowly over 5 to 10 seconds.
Pull the needle out at the same angle, then press a swab gently on the spot.
Rotate where you inject each time. Hitting the same spot over and over can cause small lumps to form under the skin over time.
TB-500 Dosage by Injury Type
Acute injuries (sprains, strains, partial tears):
Standard 4-week loading, then 4 to 8 weeks of maintenance. Most people see real change by the end of the loading phase.
Chronic tendon issues
Stretch the loading phase to 6 weeks. If improvement stalls, some practitioners run a second loading round after maintenance.
Post-surgical recovery
Wait 2 to 4 weeks after surgery, once the initial swelling has settled down, and get your surgeon's sign-off first. Run the full 12-week cycle.
More than one injury at once
This is actually where TB-500 shines, since it works systemically, one protocol covers every injury site at the same time. That's a real practical advantage over peptides that only work locally.
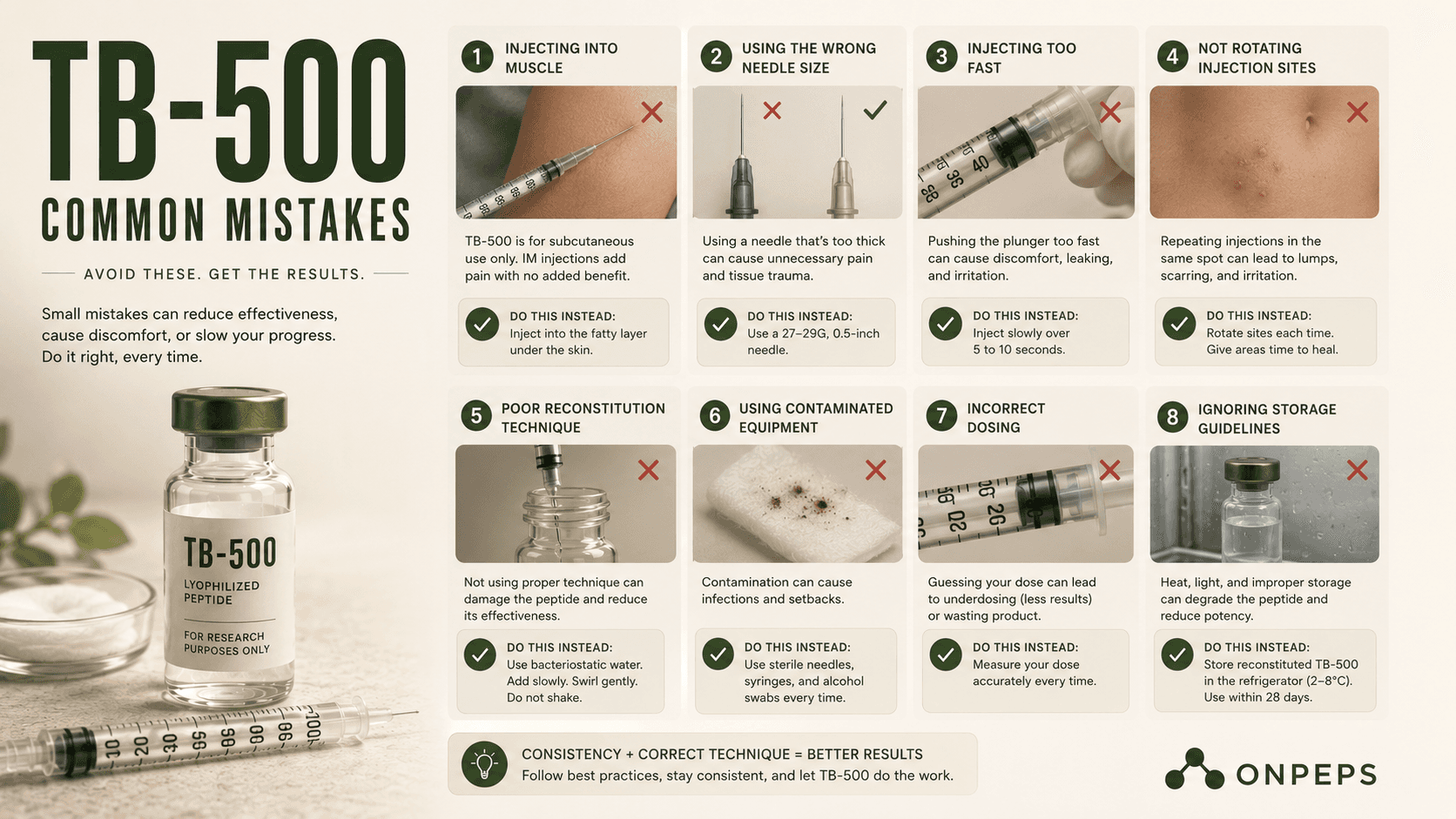
Common TB-500 Mistakes
Shaking the vial
Don't shake the vial. That's why forums are full of images of vials full of bubbles, etc. Shaking can damage the peptide structure. If you need to mix it after adding water, swirl gently.
Using regular sterile water instead of bacteriostatic water
Sterile water has no preservative, so it's only good for about 24 hours once opened. Bacteriostatic water (with 0.9% benzyl alcohol) stays safe in the fridge for 28 days.
Not refrigerating TB-500 after reconstitution
Once mixed with bacteriostatic water, TB-500 should be stored in the refrigerator at 2 to 8°C (36 to 46°F). Avoid freezing, repeated warming, or leaving the vial at room temperature for long periods, as these can reduce peptide stability.
Injecting right at the injury
That is unnecessary; see above. The abdomen works just as well no matter where the injury is.
Skipping the break between TB-500 cycles
The 4-week rest period exists because there's no long-term data on continuous use. Don't skip it just because you're impatient.
Buying TB-500 from vendors with no independent lab testing
This one matters more than people realize. FDA inspections have repeatedly found research-grade peptides with inaccurate dosing and contamination, which is actually why the FDA moved several peptides to Category 2 back in 2023.
Always check for an independent third-party Certificate of Analysis before you trust what's actually in the vial.
FAQ
Should I Take TB-500 Daily or Weekly?
There is no clinically established TB-500 dosing schedule. Most practitioner protocols use 2 to 2.5 mg twice weekly during the loading phase, while some use approximately 1 mg daily for acute injuries. Human studies have not determined which approach is superior.
Is Mega-Dosing TB-500 Worth It?
Some practitioners report using 4 to 5 mg per injection twice weekly (8 to 10 mg per week) for severe or long-standing injuries. These higher-dose protocols have not been evaluated in human clinical trials, so there is no evidence that they are more effective than standard protocols.
How Long Does TB-500 Take to Work?
Recovery times reported by users varied depending on the injury. Reported examples included:
Three hernia repairs: cleared to return to road cycling after 4 weeks instead of the expected 12 to 16 weeks.
Loose skin removal surgery: described as looking 6 weeks post-operative at the 2-week follow-up.
Broken wrist with muscle and tendon injuries: returned to light-duty work after 3 weeks instead of the expected 3 months.
Torn biceps tendon: reported healing in 3 weeks.
Broken foot: returned to the gym after 3 weeks.
ACL surgery: able to run in a straight line after 4 weeks.
Deviated septum surgery: reported minimal scarring and swelling resolving in weeks rather than months.
Appendectomy: surgeon commented on unusually fast healing at the 1-week follow-up.
Knee injury: one user reported no ongoing problems after using BPC-157 and TB-4, while another reported a long-standing hip injury did not fully heal despite using BPC-157 and TB-500.
These are individual user reports and not results from human clinical trials.
Does TB-500 Need to Be Refrigerated After Mixing?
Yes. Once reconstituted with bacteriostatic water, TB-500 should be stored in the refrigerator at 2 to 8°C (36 to 46°F). Proper storage helps maintain peptide stability during use.
Should You Inject TB-500 Directly Into the Injury?
You can, but it is generally not considered necessary. TB-500 is thought to work systemically, meaning it circulates throughout the body rather than acting only at the injection site. Subcutaneous injections into the abdomen, thigh, or upper arm are commonly used.
Resources:
Rahaman et al. (2024) — https://pubmed.ncbi.nlm.nih.gov/38382158/
Maar et al. (2025) — https://pubmed.ncbi.nlm.nih.gov/40362372/
Di et al. (2026) — https://pubmed.ncbi.nlm.nih.gov/41570941/
Zhu et al. (2016) — https://pubmed.ncbi.nlm.nih.gov/27288307/
Gao et al. (2015) — https://pubmed.ncbi.nlm.nih.gov/26083021/
Morris et al. (2018) — https://pmc.ncbi.nlm.nih.gov/articles/PMC6481613/
Kleinman and Sosne (2016) — https://www.sciencedirect.com/science/chapter/bookseries/abs/pii/S008367291630005X?via%3Dihub
Philp et al. (2003) — https://onlinelibrary.wiley.com/doi/10.1046/j.1524-475X.2003.11105.x
Xing et al. (2021) — https://pmc.ncbi.nlm.nih.gov/articles/PMC8724243/
SEER-1 Phase 3 Trial (2023) — https://pmc.ncbi.nlm.nih.gov/articles/PMC9820614/
ClinicalTrials.gov (NCT00832091) — https://clinicaltrials.gov/study/NCT00832091
Applied Sciences (2026) — https://www.mdpi.com/2076-3417/16/12/6202
He et al. (2022) — https://pmc.ncbi.nlm.nih.gov/articles/PMC9794587/
Lee and Burgess (2025) — https://pubmed.ncbi.nlm.nih.gov/40131143/
Mayfield et al. (2026) — https://pubmed.ncbi.nlm.nih.gov/41476424/
Jozwiak et al. (2025) — https://www.mdpi.com/1424-8247/18/2/185
Yuan et al. (2026) — https://www.mdpi.com/1422-0067/27/6/2876
FDA Federal Register (2026) — https://www.federalregister.gov/documents/2026/04/16/2026-07361/pharmacy-compounding-advisory-committee-notice-of-meeting-establishment-of-a-public-docket-request
WADA 2026 Prohibited List — https://www.wada-ama.org/en/resources/2026-prohibited-list
USADA — https://www.usada.org

