

There is no universally recommended human dosing protocol for BPC-157, no established cycle length, and no clinically confirmed injection frequency. BPC-157 has no FDA-approved dose. A study by Mayfield et al. (2026), in the American Journal of Sports Medicine, stated this directly: indications, dosing, frequency, and duration of treatment remain unknown.
As always, we at onpeps.com start with honesty and transparency to help you understand the current state and make informed peptide decisions.
However, there is no denying that thousands of people are using BPC-157 for a number of reasons. Not only are clinics prescribing it, but users are also injecting it for tendon repair, injury recovery, and even taking it orally for gut health. Yes, the human clinical trial evidence is lacking, but there is a silver lining emerging from years of self-experimentation.
There are clearly observable patterns: doses that keep appearing across unrelated users, cycle lengths that cluster around specific injury types, and timing decisions that reflect real physiological consistency.
We have studied over 50 use-cases to document what real people with everyday lives are actually using. We also look into how these choices are backed by science and where the evidence gap exists.
TLDR
No validated human dose exists. The figures widely used are derived from animal research and accumulated community experience.
The most consistently reported protocol is 250mcg twice daily via subcutaneous injection.
Body weight does not drive dose. Injury severity and chronicity do.
The sub-30-minute plasma half-life is the pharmacokinetic basis for twice-daily dosing, though no human study has confirmed this produces better outcomes.
Cycle lengths of 4 to 8 weeks are most common for acute injuries. Chronic and post-surgical cases often run 8 to 12 weeks or longer.
Oral dosing runs higher than injectable to compensate for reduced absorption.
Most early non-responders are not failing, they are not waiting long enough.
Why There Is No Standard BPC-157 Dose
Most approved drugs have validated dosing because they completed human trials before reaching patients. BPC-157 has not.
The only human data available comes from a 2025 pilot study by Lee and Burgess, published in Alternative Therapies in Health and Medicine. Two healthy adults received intravenous BPC-157 at 10mg, followed by 20mg the next day. No bad effects were reported. All biomarkers remained normal, and plasma levels returned to baseline within 24 hours.
Do you see what we mean when we say that human data is limited? Two people, no controls, no oral or subcutaneous data. That is the complete extent of human research on BPC-157 as of mid-2026.
Everything else comes from animal models. He et al. (2022), writing in Frontiers in Pharmacology, conducted the most thorough preclinical study across rats and beagle dogs.
They found a half-life of under 30 minutes post-injection, with bioavailability after intramuscular administration at 14 to 19 percent for rats and 45 to 51 percent for dogs. Excretion occurred primarily via urine and bile. The peptide disappeared from plasma within 4 hours.
Because rats and dogs absorb this drug so differently, we cannot rely on their results to predict how it works in humans. We have no data on human absorption, which is why usage protocols vary so much. Without human trials, every approach is an estimate.
User 22 in our observational data highlighted this uncertainty when questioning if he really wanted to continue dosing twice daily in light of the 30-minute half-life. He proposed that a single 500mcg injection could be equally effective. However, this is up for debate. So it can't be said for certain if his idea was right or wrong.
What BPC-157 Doses Are Being Used Today
Without official human research, three things dictate current dosing.
First, translations of animal study data,
then long-standing patterns established by experimental usage and mentioned in forums
and lastly, specific protocols used by clinics and compounding pharmacies.
Across those sources, a consistent range has emerged for subcutaneous or under-the-skin injections.
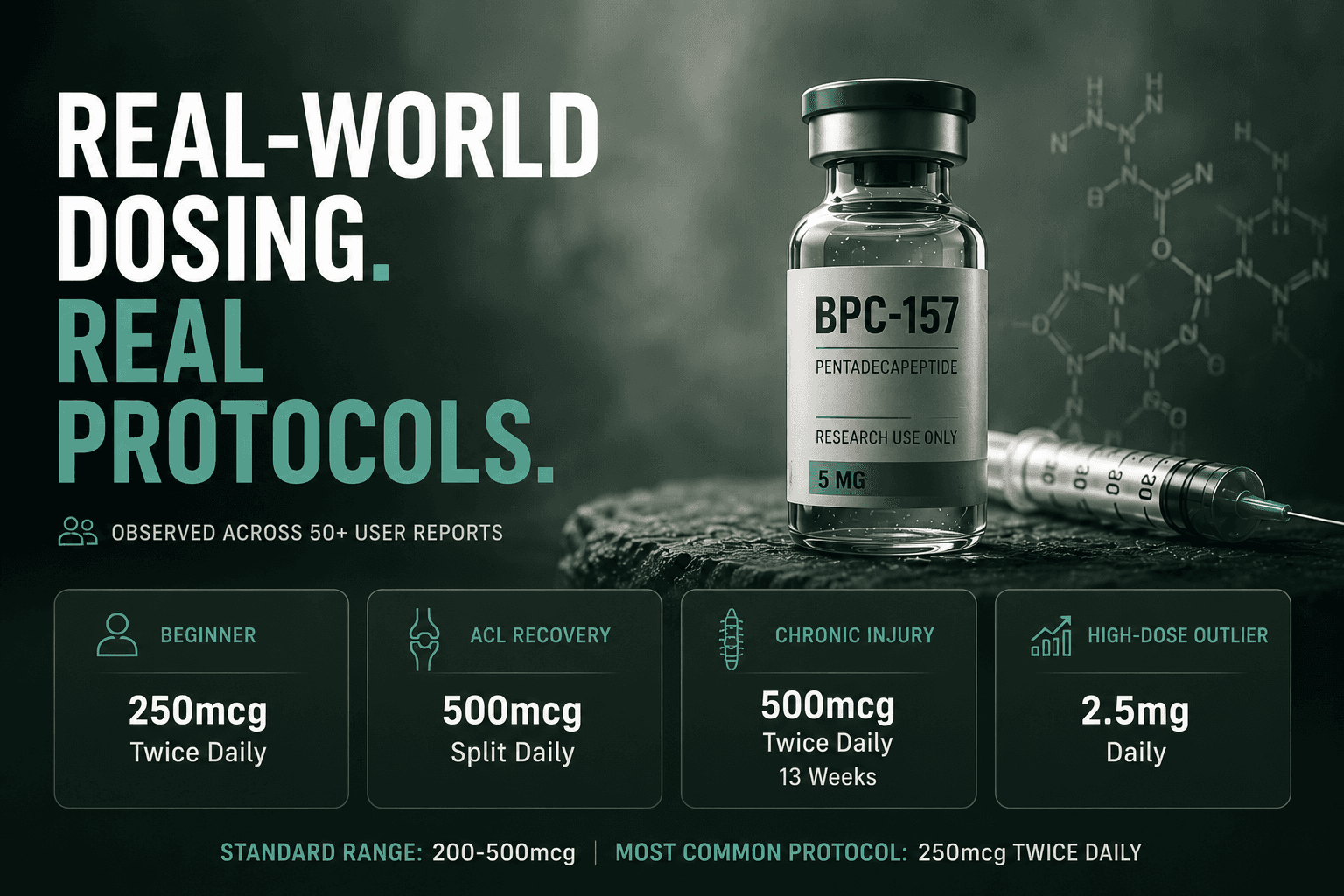
Standard range: 200 to 500mcg once or twice daily
The most commonly reported protocol across all sources is 250mcg twice daily. This appears in licensed clinic protocols, documented procedures from 503A compounding pharmacy providers, and the majority of user reports in our observational data.
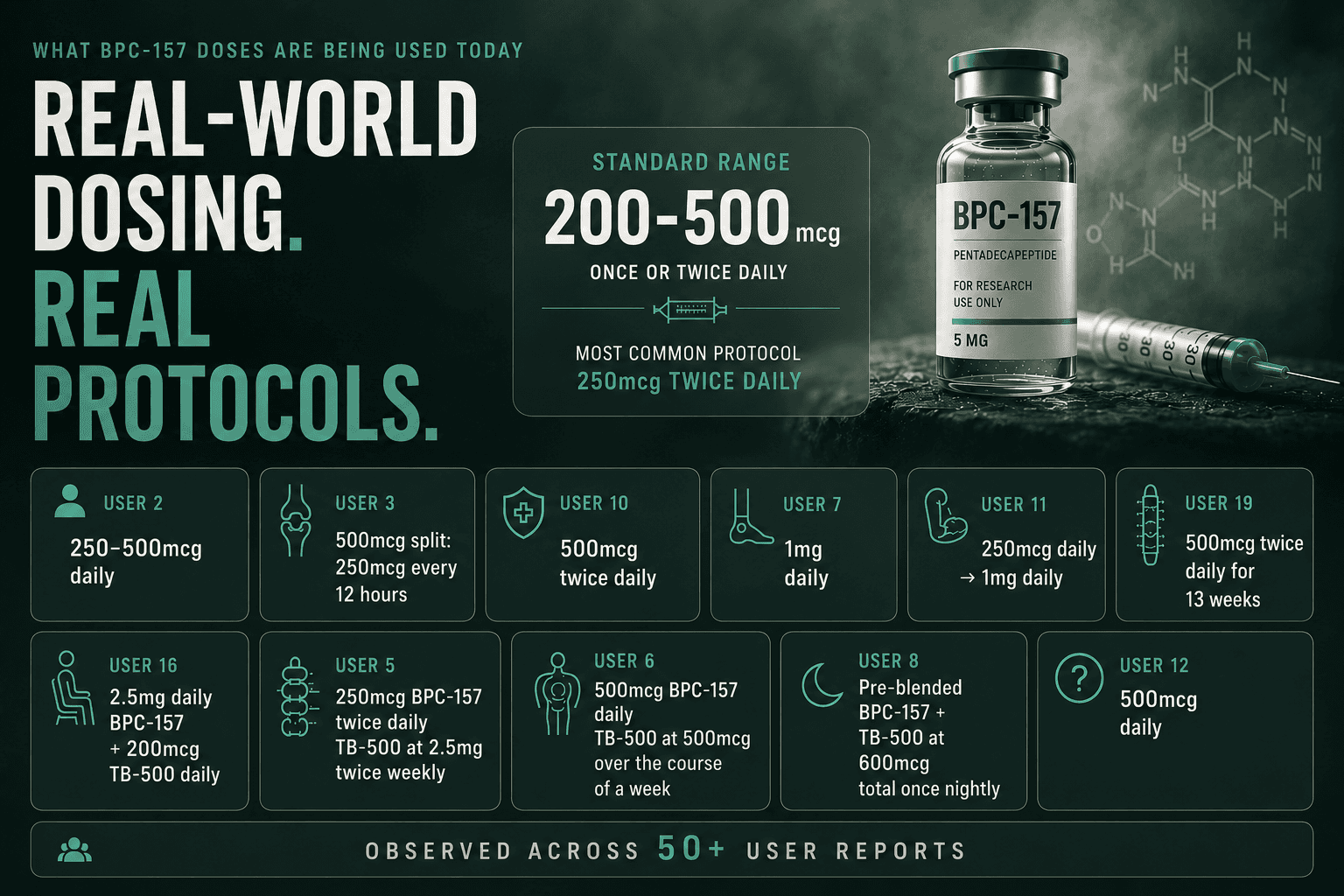
User 2 followed exactly this structure for a 12-week beginner protocol, running 250 to 500mcg daily during the loading phase and dropping to 250mcg daily for maintenance.
User 3, recovering from a complete ACL and LCL rupture at 21 years old, used 500mcg split as 250mcg every 12 hours and discontinued at day 40. The results were so extraordinary that even his surgical team was astounded.
User 10, a 43-year-old recovering from ACL revision and Grade 3 meniscus repair, ran 500mcg twice daily. He did so once on an empty stomach in the morning and once roughly three hours after his final meal. He began three days before surgery and continued every day post-operatively. His physiotherapist placed his recovery in the top 3 to 5 percent of comparable cases.
There are also cases of the higher range of 500mcg being used twice daily. User 7 started using 1mg daily for the acute phase following major foot surgery, planning to reduce afterward.
User 11 started at 250mcg daily for golfer's elbow and progressed to 1mg daily after finding insufficient response at the lower dose.
User 19 ran 500mcg twice daily for 13 weeks across a chronic multi-injury case involving a 10-year back injury and a 4-year shoulder injury, adding GHK-Cu, ipamorelin, and CJC-1295 to the protocol, and reported 90 percent pain relief after one cycle.
User 16, a 68-year-old woman bedridden with L5 spinal stenosis and scoliosis, used an unusually high BPC-157 dose of 2.5mg daily alongside 200mcg TB-500 daily, transitioning the TB-500 to every third day after two weeks. She reported complete pain resolution at five weeks.
Several other users in the dataset reported protocols worth noting.
User 5, a 36-year-old with two herniated discs on his first peptide cycle, started with 250mcg BPC-157 twice daily alongside TB-500 at 2.5mg twice weekly. This is the most commonly referenced beginner structure.
User 6, dealing with chronic back and shoulder pain, went with 500mcg BPC-157 daily alongside TB-500 at 500mcg over the course of a week. But he was also cautious about whether TB-500 at that level was correct, given the different dosing needs of each compound.
User 8, a 22-year-old with Grade 1 tears across multiple sites, used a pre-blended BPC-157 and TB-500 product at 600mcg total once nightly.
User 12 used 500mcg daily and was specifically trying to determine whether splitting that dose or taking it all at once produced better results. Many of these are questions that remain unanswered in human research.
Across the aggregate dosing patterns observed, one protocol that appeared in multi-injury ACL contexts was a 750mcg daily blend of BPC-157 and TB-500 combined.
Animal Research Context
Published preclinical studies typically use 2.5 to 10mcg per kilogram of body weight. For a 75 to 90kg adult, that translates roughly to 190 to 900mcg daily, which brackets the 200 to 500mcg range being used in practice.
Oral Dosing Runs Higher
Injectable: 200 to 500mcg per dose
Oral: 500 to 1,000mcg per dose, once or twice daily, taken on an empty stomach
Higher oral doses are used to make up for the fact that the gut absorbs the compound poorly compared to injections. There is no precise data on this ratio for humans. For more on oral versus injectable administration, see our next article, the BPC-157 Administration Guide.
Real-World BPC-157 Protocol Snapshot
Across the broader observational dataset, we noticed some similar patterns:
Protocol Type | Typical Dose | Common Duration | Primary Use Case |
|---|---|---|---|
Conservative injectable | 250mcg once daily | 4 to 6 weeks | Chronic tendon, maintenance |
Standard injectable | 250mcg twice daily | 6 to 8 weeks | Active musculoskeletal injury |
Aggressive injectable | 500mcg twice daily | 2 to 4 weeks acute, longer for chronic | Acute injury, post-surgical, chronic multi-injury |
Oral capsule | 500 to 1,000mcg daily | 4 to 8 weeks | Gut health, injection avoidance |
Combined stack (BPC + TB-500) | 250 to 500mcg BPC + 1 to 2mg TB-500 | 6 to 12 weeks | Chronic degeneration, complex injury |
These are observational patterns, not recommendations.
Body Weight and BPC-157 Dosing: What Users Found
One of the most persistent questions in peptide communities is whether heavier individuals need higher doses.
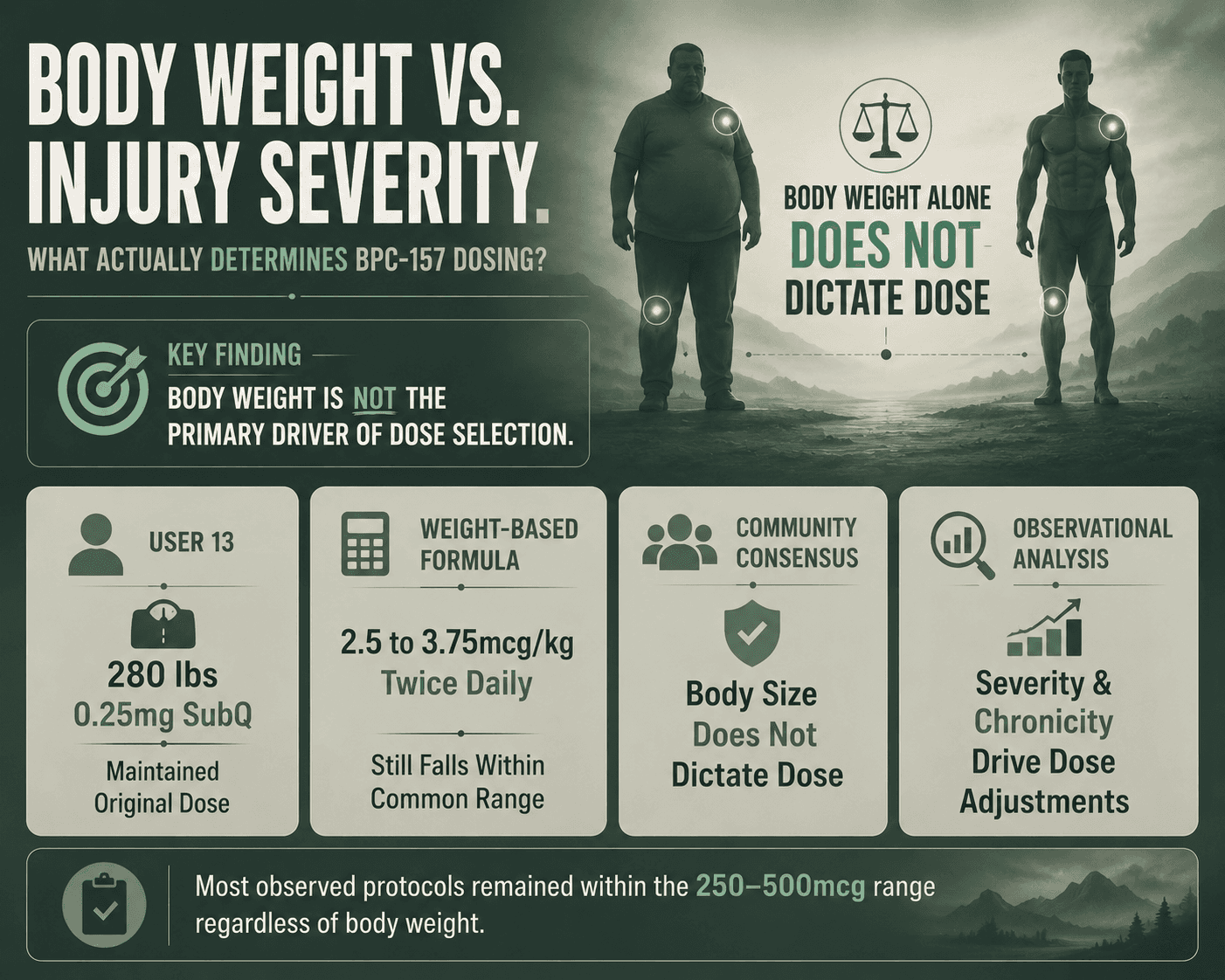
User 13, at 280 pounds, specifically questioned whether his 0.25mg subcutaneous dose was insufficient given his body weight. He was considering adding 0.5mg oral BPC-157 on top, but ended up sticking to the dosage after some discussion within the peptide community.
More experienced users maintain the opinion that it is not about body weight. They think the efficacy of BPC-157 is directly affected by the extent of the injury.
Across our broad dataset, injury severity and chronicity were the primary dosing variables that kept appearing, not body size. This fits the science: BPC-157 uses signaling pathways that stop responding once they reach a certain level. Increasing the dose beyond the effective range adds little benefit regardless of body weight.
User 15 cited a general dosing range of 2.5 to 3.75mcg per kilogram of body weight twice daily, which, at higher body weights, still produces doses within the standard 250 to 500mcg range being used across the dataset.
User 15 also calculated the total quantities needed for a full 3-month cycle: 45mg of BPC-157 total (at 0.5mg daily over 90 days) and approximately 65mg of TB-500 total (5mg twice weekly for the loading week, then 2.5mg twice weekly for the remaining 11 weeks). These figures are useful for purchasing decisions before starting.
Body Weight vs. Injury Severity Dosing Data for BPC-157
User / Source | Body Weight / Context | Dosing Context & Decisions | Observational Findings & Rationale |
User 13 | 280 lbs | Questioned if a 0.25mg subcutaneous dose was insufficient for his size; considered adding 0.5mg oral BPC-157. | Maintained his original dosage after community consultation. Highlights the misconception that heavy body weight requires escalated doses. |
User 15 | Various (Calculated per kg) | Cited a general dosing range of 2.5 to 3.75mcg per kilogram taken twice daily. | Even at significantly higher body weights, this formula still lands doses within the standard 250 to 500mcg dataset baseline. |
Experienced Users | Broad Community Consensus | Argued that body weight is irrelevant to efficacy. | Maintained that dosing should be dictated by the extent and severity of the injury, not body size. |
Observational Dataset Analysis | Broad Systemic Tracking | Evaluated body weight vs. primary dosing variables. | Confirmed that injury severity and chronicity are the true drivers of dose adjustments. This aligns with the fact that cells can only process so much of the signal at once. |
BPC-157: Take It Once Daily or Split - The Half-Life Question
The sub-30-minute plasma half-life documented in He et al. (2022) creates a specific problem for dosing frequency. If you inject only once a day, the peptide disappears from your system for most of that 24-hour window.
This is the basis for twice-daily dosing. User 3 split his 500mcg dose as 250mcg every 12 hours specifically to account for what he cited as a 4 to 6-hour half-life. User 10 timed his two daily doses around meals for similar reasons.
But when we looked at the data of User 22, we found a legitimate contradiction. If the half-life is genuinely under 30 minutes, the compound is cleared too rapidly. This means that even twice-daily dosing leaves long windows without measurable peptide.
We do not know if the body needs a constant supply of the peptide to heal, or if a quick pulse is enough to trigger a self-sustaining healing process. No human study has ever tested this.
What the observational data reveal is that many users ran once-daily protocols and still reported meaningful recovery. Whether twice-daily dosing produced better outcomes cannot be determined from self-reported data alone.
The current community consensus, reflected in clinic protocols and forum guidance alike, is to split doses where possible. It is a reasonable precaution in the absence of evidence either way.
BPC-157 Timing, Empty Stomach, and Days Per Week
Empty stomach
One thing we noted was that orally, BPC-157 was taken consistently on an empty stomach. The reasoning is simple: avoid competition with food digestion. The intention is also to allow the peptide to come directly in contact with the gut lining.
User 2 specifically noted morning dosing on an empty stomach as part of his protocol structure.
For injections, food timing doesn't matter because the peptide bypasses the digestive tract entirely. User 10 used morning injection on an empty stomach and evening injection roughly three hours after his last meal. But this was just a personal choice.
Time of Day
There is no evidence that there is an optimal injection time in humans. Morning injection is the most common pattern across reported protocols, mainly influenced by convenience, lifestyle, and routine.
User 2 used morning timing throughout his 12-week protocol. User 3 split AM and PM doses evenly.
Days Per Week
This is where things got interesting because there were a lot of conflicting opinions. But overall, the dominant pattern seems to be daily administration.
Some users run five days on, two days off, treating it similarly to training schedules. No evidence suggests this produces meaningfully different outcomes compared to seven-day dosing.
The primary recommendation across clinic frameworks and experienced users is consistency over precision. It is more important to maintain a dosing pattern than to miss occasional doses.
Weekly Schedule
For the standard Wolverine Stack, the most commonly used structure across the dataset is:
Weeks 1 to 4 (Loading)
Day | BPC-157 | TB-500 | Notes |
|---|---|---|---|
Monday | 250mcg (10 units) | 2.5mg (50 units) | Both injections |
Tuesday | 250mcg (10 units) | — | BPC only |
Wednesday | 250mcg (10 units) | — | BPC only |
Thursday | 250mcg (10 units) | 2.5mg (50 units) | Both injections |
Friday | 250mcg (10 units) | — | BPC only |
Saturday | 250mcg (10 units) | — | BPC only |
Sunday | 250mcg (10 units) | — | BPC only |
Weeks 5 to 12 (Maintenance)
Day | BPC-157 | TB-500 | Notes |
|---|---|---|---|
Monday | 250mcg (10 units) | 2.5mg (50 units) | Both injections |
Tuesday | 250mcg (10 units) | — | BPC only |
Wednesday | 250mcg (10 units) | — | BPC only |
Thursday | 250mcg (10 units) | — | BPC only |
Friday | 250mcg (10 units) | — | BPC only |
Saturday | 250mcg (10 units) | — | BPC only |
Sunday | 250mcg (10 units) | — | BPC only |
If a dose was missed, the advice is to dose the next day, not double up.
Progress Tracking
Tracking weekly is the most reliable way to assess whether a protocol is working, particularly given the delayed response timeline. A simple weekly log:
Week number:
Date:
Primary injury or goal:
Pain level (1 to 10):
Mobility and function (1 to 10):
Sleep quality (1 to 10):
Side effects if any:
Notes:
Specific things worth tracking: how long you can perform a given activity before pain starts, range of motion changes, morning stiffness, and workout recovery time. Photos are useful for anything with a visual component.
BPC-157 Cycle Lengths by Injury Type
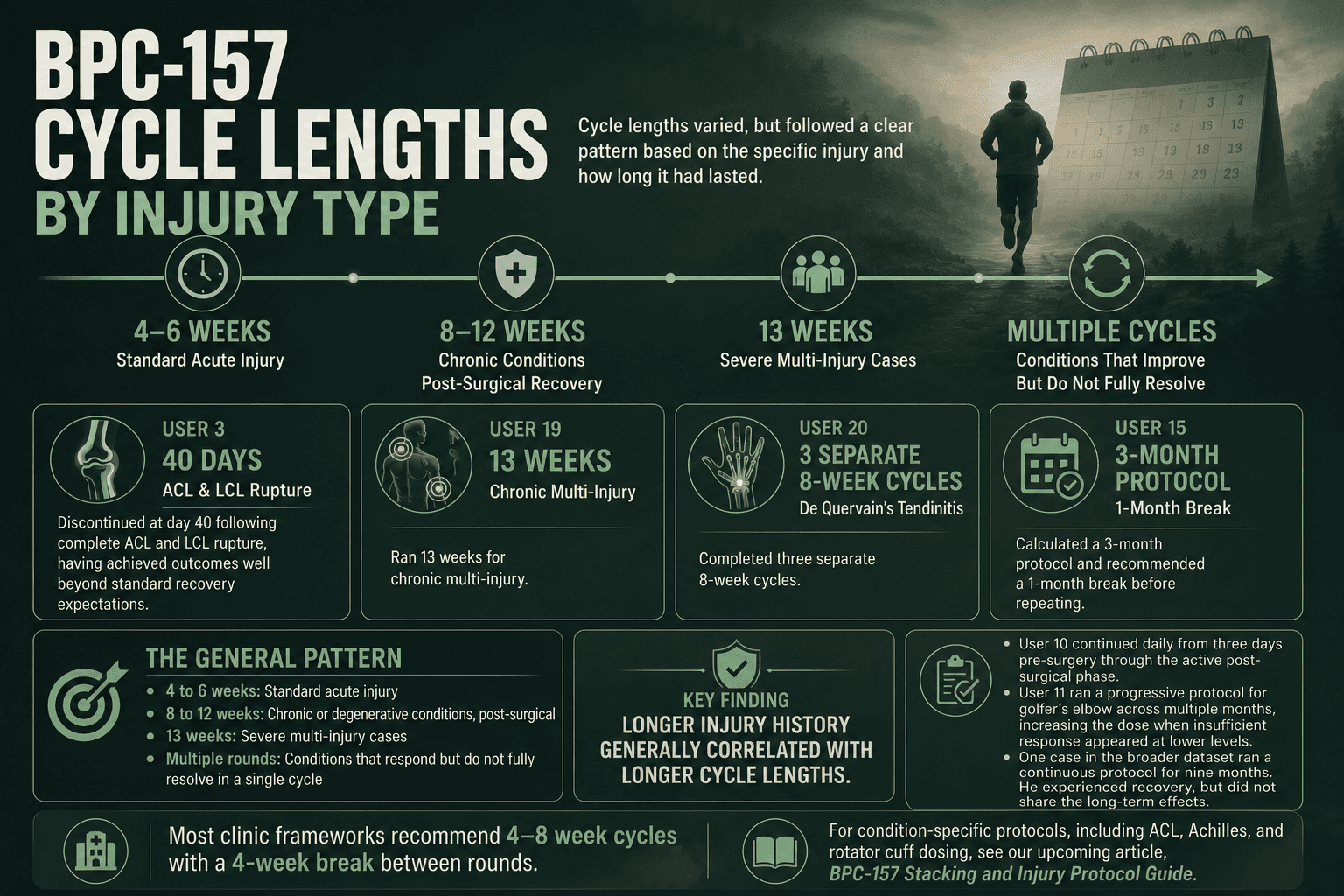
There was significant variety in cycle lengths, but it followed a clear pattern based on the specific injury and how long it had lasted.
Acute Injuries and Post-Surgical Recovery
User 3 discontinued at day 40 following complete ACL and LCL rupture, having achieved outcomes well beyond standard recovery expectations.
User 10 continued daily from three days pre-surgery through the active post-surgical phase. The broad pattern for acute injuries and post-surgical contexts in the data sits between four and eight weeks.
Chronic and Degenerative Conditions
User 11 ran a progressive protocol for golfer's elbow that extended across multiple months, increasing the dose when insufficient response appeared at lower levels.
User 19 ran 13 weeks for chronic multi-injury.
User 20 ran three separate 8-week cycles for De Quervain's tendinitis.
User 15 calculated a 3-month protocol and recommended a 1-month break before repeating.
One case in the broader dataset ran a continuous protocol for nine months. While he experienced recovery, he also didn't share the long-term effects.
The general pattern
4 to 8 weeks: Standard for acute injury in real-world users.
Finishing phase (weeks 9 to 12): BPC-157 continues at 250mcg daily, TB-500 at 2.5mg once weekly. The purpose is maintaining optimal levels while the body completes the deeper structural repair that takes longest. Feeling better is not a reason to stop early — the real rebuilding often happens in this final phase.
8 to 12 weeks: Chronic or degenerative conditions, post-surgical
13 weeks: Severe multi-injury cases
Multiple rounds: Conditions that respond partially but do not fully resolve in a single cycle. Clinic frameworks typically recommend 4 to 8 weeks for most conditions with a 4-week break between cycles. Severe tendon cases, including Achilles and rotator cuff pathology, are often extended to 8 to 12 weeks.
For condition-specific protocols, including ACL, Achilles, and rotator cuff dosing, see our upcoming article, BPC-157 Stacking and Injury Protocol Guide.
When to Expect Results after Using BPC-157
The most predictable behavior was increased dosage following a lack of early results. If users saw no change in the first 14 days, they routinely bumped up their dose, switched injection sites, or questioned if their peptide was real.
Most of the time, they were not failing. They were not waiting long enough.
Real-world Response Timeline across BPC-157 Injectable Protocols
Days 1 to 5: Most users reported little to no change, while some noted mild injection-site redness. This is the period where premature dose escalation most commonly occurred.
Weeks 1 to 2: Signs of improvement show up as faster recovery between workouts and lower post-training soreness. User 17 reported that three years of nightly carpal tunnel pain ended within one month.
User 18 reported ten years of knee pain cleared in three days while using the "Wolverine Stack." This is an extreme case, but it highlights that results depend heavily on the person.
Weeks 2 to 4: Stronger responders notice physical changes, including better range of motion, fewer flare-ups, and the ability to handle more physical load. User 3 reached full mobility by day 20 and resumed running by day 30.
Weeks 4 to 8: Improvements either plateau or persist. User 16 reported being pain-free at week 5, moving from a bedridden state caused by L5 stenosis to full recovery.
Post-discontinuation: Many users reported ongoing benefits after stopping. User 3 was still gaining ground at week 8, three weeks after ending the cycle at day 40.
Oral protocols
Results from oral use are less noticeable and take longer to start than those from injections. Gut-related benefits generally show up in two to four weeks instead of days.
Dose Escalation and the Non-Response Problem
Most users do not find that BPC-157 acts as a painkiller. It works by supporting tissue repair, which takes time.
Because there is no proven human dose limit, users often guess. User 21 is a cautionary case: his first vial worked, but his next two caused diarrhea, dizziness, nausea, and headaches.
The community generally attributes this to poor manufacturing. And higher doses have also occasionally been linked to eye issues that do not occur at lower levels. If you increase your dose to get results, you are also increasing your exposure to potentially impure substances. You may just be taking more of a bad product.
Breaks Between BPC-157 Cycles
User 15 explicitly recommended up to 3 months of BPC-157 followed by a 1-month break. Clinic frameworks typically follow a similar pattern, recommending a break of roughly equal length.
The goal is to preserve receptor sensitivity and let the body consolidate its progress instead of using the compound long-term.
Because many users report continued healing weeks after finishing a cycle, it confirms that the biological repair triggered by the peptide continues after discontinuation. This might be one of the best arguments as to why there needs to be more human trials.
It is unproven whether BPC-157 causes receptor downregulation in humans. The recommendation to cycle off is based on caution, not hard evidence.
User 20 ran three separate 8-week cycles for De Quervain's tendinitis, suggesting that repeat cycles are used when conditions respond partially but do not fully resolve. One case in the dataset ran continuously for nine months without a reported break, representing the far end of observed behavior.
Key Takeaways
BPC-157 has no FDA-approved dose and no validated human dosing protocol. The 200 to 500mcg figures widely used across clinic and community contexts are derived from animal extrapolation and accumulated self-experimentation, not controlled human trials.
Body weight does not determine dose. Injury severity and chronicity do.
The sub-30-minute half-life documented in preclinical research provides a pharmacokinetic rationale for twice-daily dosing. Whether it produces meaningfully better outcomes than once-daily dosing in humans remains unknown.
Oral and injectable routes serve different purposes and use different dose ranges.
Cycle lengths of 4 to 8 weeks appear most commonly for acute injuries. Chronic tendon conditions and post-surgical recovery often require 8 to 12 weeks or multiple cycles before meaningful structural change becomes apparent.
Early non-response is not failure. Most users who escalated doses in the first one to two weeks were doing so before sufficient time had passed for structural recovery to manifest.
The 2026 regulatory changes opened a path toward licensed compounding access in the United States, but the FDA's Pharmacy Compounding Advisory Committee decision in July 2026 will determine whether that path expands or narrows. WADA prohibition remains in force for tested athletes regardless of regulatory changes elsewhere.
Read BPC-157 Peptide Therapy for Tendon Repair, Shoulder Injuries, Tennis Elbow & Achilles Recovery and BPC-157 and the Brain-Gut Axis: Gut Integrity, Systemic Inflammatory Signaling, and the Science of Gastrointestinal Repair for a deeper understanding backed by science.
FAQ
What is the standard starting BPC-157 dose?
The most common protocol is 250mcg twice a day, injected under the skin. Some users start with 250mcg once a day. Since no human clinical trials exist, these numbers are based on animal research and years of community experience.
Does body weight change the BPC-157 dose?
No. Reported experience suggests that injury severity and how long the injury has lasted matter more than body weight. A 280-pound person and a 160-pound person often use the same dose. The theory is that the body’s signaling pathways reach their limit at low concentrations regardless of body size.
Is 250mcg BPC-157 too low?
Not necessarily. Many users report success at 250mcg for mild to moderate injuries. Those with severe or long-term issues often increase their dose later. It is generally recommended to start low and see how your body reacts before increasing.
Why inject peptide twice a day?
Research shows the peptide leaves the bloodstream in under 30 minutes. Injecting twice a day keeps the levels more stable throughout the day. However, it is not proven if this actually leads to better results in humans.
Is 1mg BPC-157 per day too much?
Some users have taken 1mg daily for severe injuries without reporting major issues, and others have used even more. There is no officially safe maximum limit for humans. While one pilot study showed two people tolerating 20mg intravenously, that does not guarantee that long-term daily injections are safe.
How long before peptides start working?
Don't expect much in the first week. Basic improvements usually appear by weeks one to two. Better movement and fewer flare-ups typically show up between weeks three and four. Oral versions work even slower, taking two to four weeks to help with gut issues.
Is 4 weeks enough time for BPC-157 to work?
Four weeks might work for a fresh injury, but it is often too short for chronic, long-term conditions. Many successful recoveries take eight to twelve weeks. Quitting at four weeks just because you haven't seen a massive change is a common mistake.
Should I take breaks from taking BPC-157?
Yes. Experienced users and clinic protocols recommend taking breaks. A common method is to take a break as long as the cycle itself. The theory is that this keeps your body sensitive to the peptide and helps you lock in your progress, though this hasn't been proven.
How do I calculate my BPC-157 dose from a 10mg vial?
If you add 2ml of bacteriostatic water to a 10mg vial, you have 5,000mcg per ml. On a standard U-100 insulin syringe, 10 units equals 500mcg, and 5 units equals 250mcg. If you use a different amount of water, divide the total micrograms by the milliliters of water to find your strength. See our [BPC-157 Administration Guide] for full instructions.
Why are there so many different protocols?
Because no official human dosing study exists. Every protocol you see, whether from a doctor, a website, or a study, is an educated guess based on animal data or trial-and-error. Different injuries and goals lead people to try different things. This uncertainty is standard for the world of experimental peptides.
Resources:
He et al. (2022) — https://pmc.ncbi.nlm.nih.gov/articles/PMC9794587/
Lee and Burgess (2025) — https://pubmed.ncbi.nlm.nih.gov/40131143/
Mayfield et al. (2026) — https://pubmed.ncbi.nlm.nih.gov/41476424/
Jozwiak et al. (2025) — https://www.mdpi.com/1424-8247/18/2/185
Yuan et al. (2026) — https://www.mdpi.com/1422-0067/27/6/2876
FDA Federal Register (2026) — https://www.federalregister.gov/documents/2026/04/16/2026-07361/pharmacy-compounding-advisory-committee-notice-of-meeting-establishment-of-a-public-docket-request
WADA 2026 Prohibited List — https://www.wada-ama.org/en/resources/2026-prohibited-list
USADA — https://www.usada.org/spirit-of-sport/bpc-157-peptide-prohibited/

