

TB-500 and BPC-157 are the two peptides people combine most often for injury recovery, but they don't work the same way and they're not interchangeable. Picking between them, or stacking them, should come down to how each one actually works, not just habit or whatever you've seen other people running.
Quick Comparison
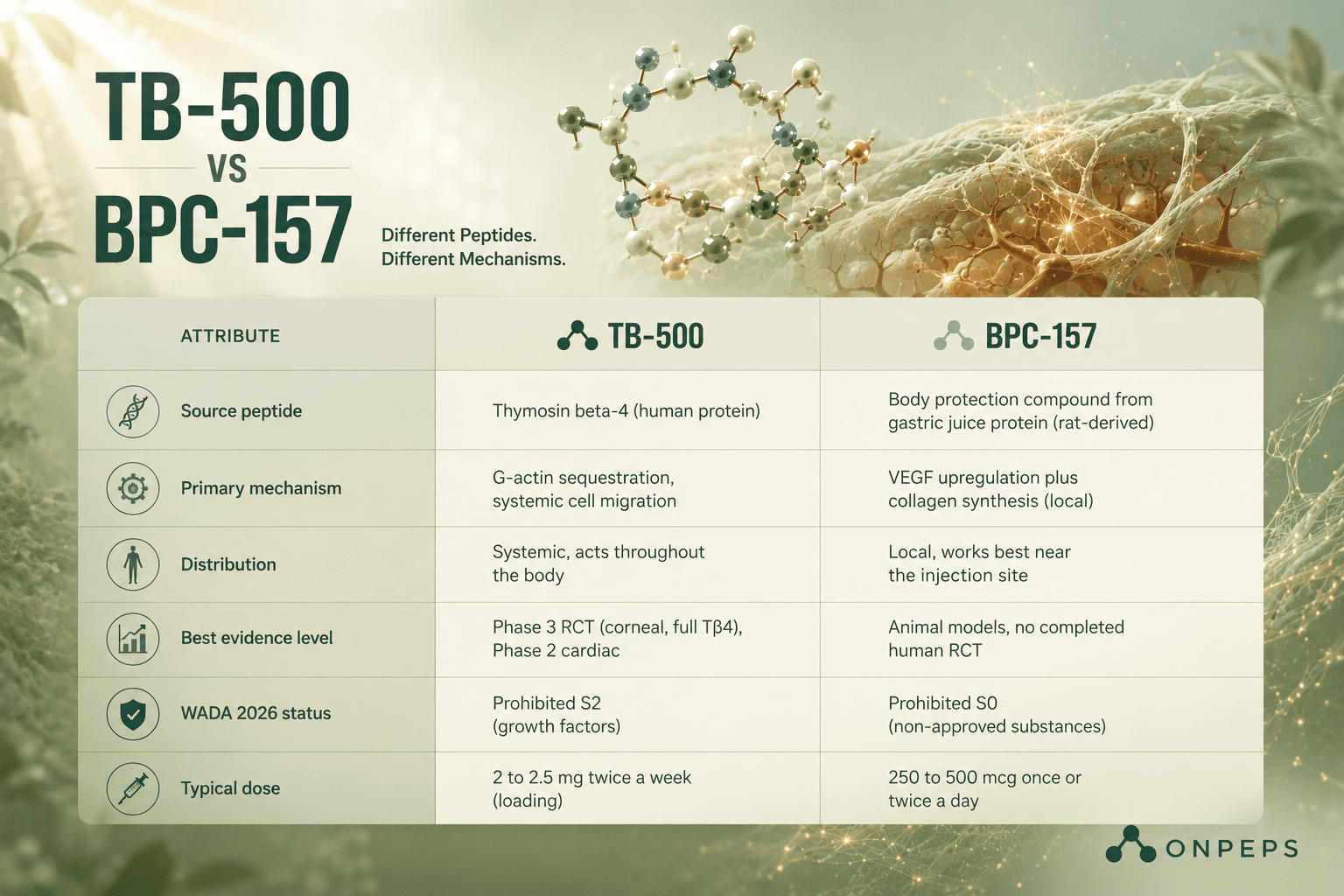
Attribute | TB-500 | BPC-157 |
Source peptide | Thymosin beta-4 (human protein) | Body protection compound from gastric juice protein (rat-derived) |
Primary mechanism | G-actin sequestration, systemic cell migration | VEGF upregulation plus collagen synthesis (local) |
Distribution | Systemic, acts throughout the body | Local, works best near the injection site |
Best evidence level | Phase 3 RCT (corneal, full Tβ4), Phase 2 cardiac | Animal models, no completed human RCT |
WADA 2026 status | Prohibited S2 (growth factors) | Prohibited S0 (non-approved substances) |
Typical dose | 2 to 2.5 mg twice a week (loading) | 250 to 500 mcg once or twice a day |
How DO TB-500 & BPC-157 Work?
BPC-157 is a synthetic 15-amino acid peptide derived from a protein found in gastric juice. It mainly works by boosting VEGF and collagen synthesis right where you inject it. It also affects nitric oxide signaling and activates growth hormone receptors to support local tissue repair. It works best close to the injured tissue. For gut healing specifically, taking it orally or intraperitoneally puts the peptide in direct contact with the gut lining.
TB-500 works differently. It binds to G-actin, which speeds up cell migration throughout the entire body. Because it circulates systemically, it can act on every active injury site at once. This is the main advantage TB-500 has over BPC-157 for injuries in multiple locations or in spots that are hard to inject near.
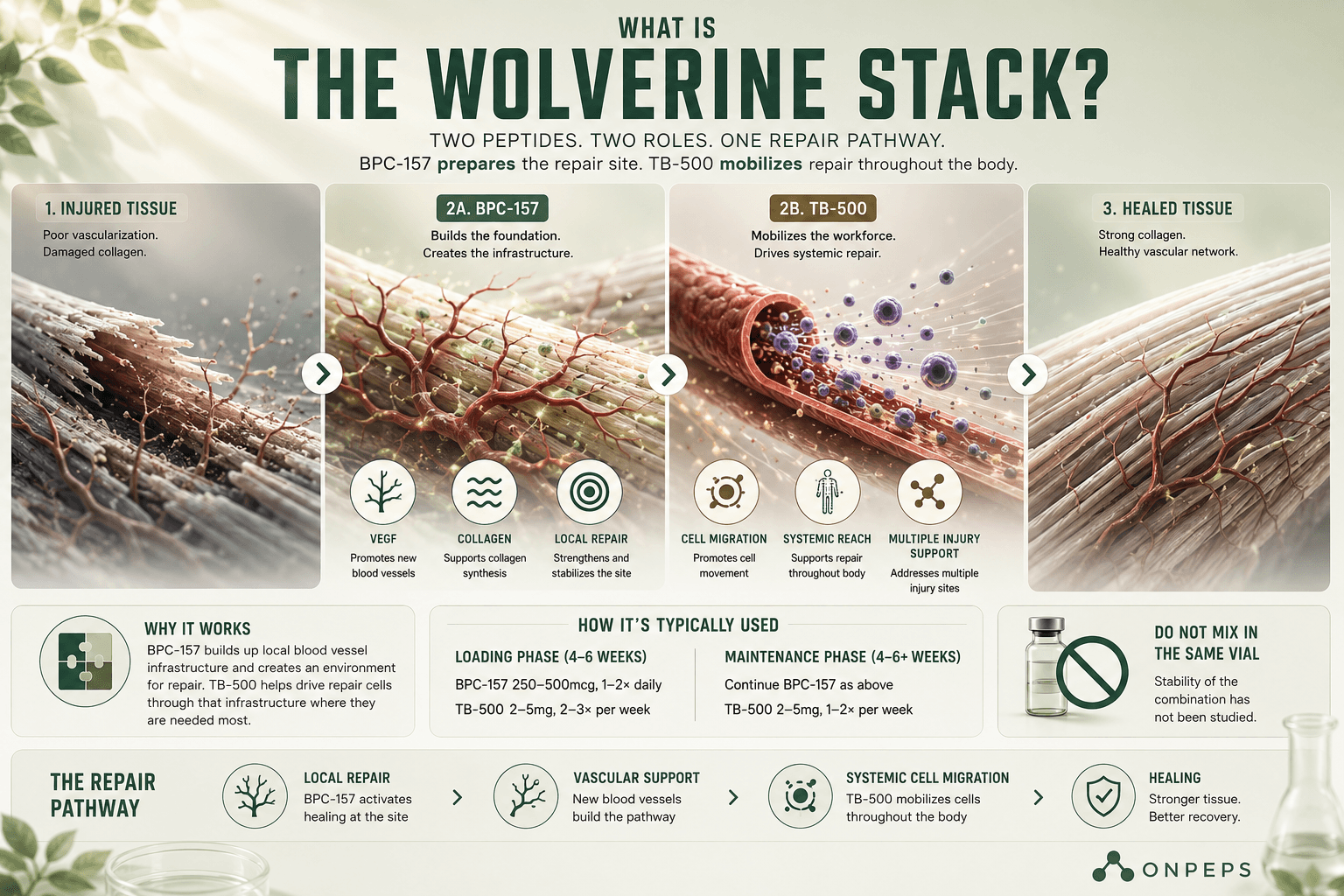
In a way, they cover sequential steps in the same repair process. BPC-157 builds up local blood vessel infrastructure, then TB-500 helps drive repair cells through that infrastructure. That's the basic reasoning behind stacking them.
When to use TB-500 & BPC-157?
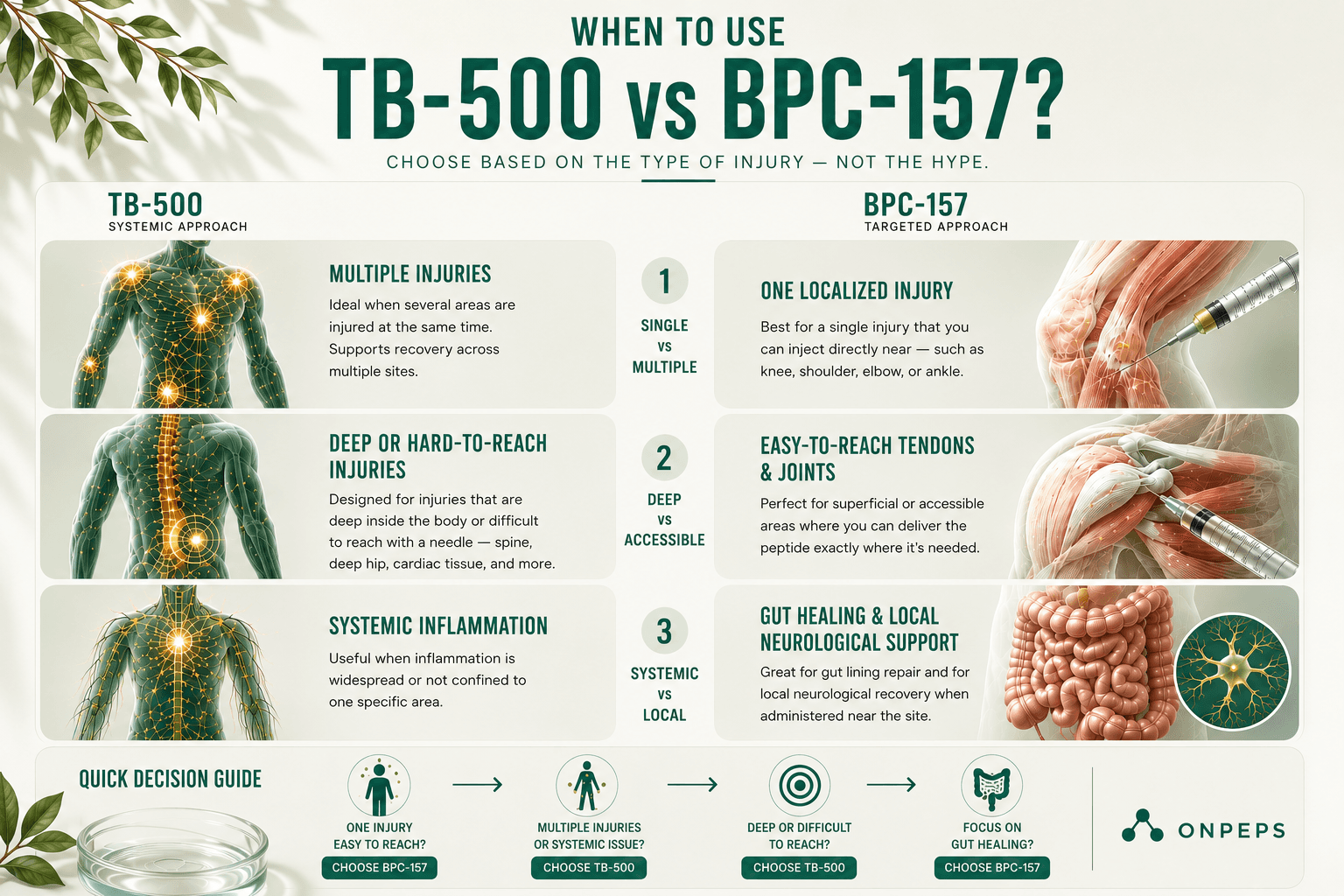
TB-500 makes more sense when:
The injury is deep or hard to reach with an injection (spine, deep hip, cardiac tissue)
You're dealing with multiple injuries at the same time
Recovery involves systemic inflammation rather than something localized
BPC-157 makes more sense when:
The injury is easy to inject near (knee, shoulder, elbow, ankle)
Gut healing is the main goal, since BPC-157's strongest documented effects are in the GI tract
You're targeting a neurological issue through a localized administration route
Neither peptide has human RCT data for musculoskeletal use yet. Choosing based on which one has more animal evidence is reasonable; the clinical gap is roughly the same for both.
Where Things Stand Legally for peptides BPC-157 & TB-500 in 2026
Both peptides were removed from the FDA's Category 2 list, but through different processes and on different timelines. TB-500's removal happened in April 2026 after the original nominators withdrew their submissions. BPC-157 followed a separate procedural path. Both are now facing their own PCAC reviews for potential Category 1 placement.
On WADA's 2026 Prohibited List, BPC-157 falls under S0 (Non-Approved Substances), while TB-500 falls under S2, the peptide hormones and growth factors section. The S2 classification reflects TB-500's structural connection to thymosin beta-4 and its documented growth factor activity. Either way, both result in the same prohibition for athletes.
What is The Wolverine Stack?
The "Wolverine stack" combines BPC-157 and TB-500 in the same protocol. The name comes from the dual-mechanism approach, BPC-157 building local vascular infrastructure paired with TB-500's systemic cell migration support.
Stack protocol:
BPC-157:
250 to 500 mcg subcutaneous, once or twice a day
Inject near the injury when you can reach it
TB-500:
2 to 2.5 mg subcutaneous, twice a week (loading phase)
Inject away from the injury, lower abdomen or outer thigh works fine
2 mg once a week (maintenance phase)
Both run at the same time through the loading phase. People often keep BPC-157 going daily through the whole cycle while TB-500 shifts into maintenance.
Can you mix TB-500 and BPC-157 in the same vial? No. Reconstitute and store them separately. They have different concentration needs, and nobody's studied whether the combined solution stays stable.
Choosing One Without Stacking
For a single acute tendon injury that's easy to inject near, BPC-157's local delivery is a reasonable first move. You can always add TB-500 later if the local approach isn't producing enough improvement, or if you need systemic coverage.
For post-surgical recovery, systemic inflammation, or injuries in multiple spots, go with TB-500 first, or combine both if your budget allows.
For gut or GI healing, stick with BPC-157 only. TB-500 doesn't have a meaningful evidence base for gastrointestinal use.
If you're an athlete worried about WADA, both are prohibited either way.
FAQ
Can TB-500 and BPC-157 be used together?
Yes, many people stack them because they work through different biological mechanisms.
Is the Wolverine Stack scientifically proven?
No, it is based on preclinical evidence and user practice rather than human clinical trials.
Which peptide is better for tendon injuries?
BPC-157 is generally preferred for localized tendon injuries that are easy to inject near.
Which peptide is better for multiple injuries?
TB-500 is typically chosen because it acts systemically.
Can TB-500 reach injuries without injecting near them?
Yes, it circulates throughout the body rather than acting only at the injection site.
Does BPC-157 have to be injected near the injury?
Local administration is commonly used because its effects appear strongest close to the target tissue.
Is TB-500 effective for gut healing?
Current evidence does not support TB-500 as a primary peptide for gastrointestinal repair.
Can BPC-157 be taken orally?
Oral formulations are mainly discussed for gastrointestinal applications, but research remains limited.
Can you mix TB-500 and BPC-157 in the same syringe?
They can be injected during the same session, but they should not be mixed in the same vial.
Can TB-500 and BPC-157 be reconstituted together?
No, they should be reconstituted and stored separately.
Which peptide has stronger human evidence?
Thymosin beta-4 has human clinical data, but TB-500 itself does not have completed human musculoskeletal trials.
Does BPC-157 have any completed human clinical trials?
No, there are currently no completed human RCTs for musculoskeletal use.
Are TB-500 and BPC-157 approved medications?
No, neither peptide is approved for general therapeutic use.
Are TB-500 and BPC-157 banned in sport?
Yes, both are prohibited under the 2026 WADA Prohibited List.
Can TB-500 replace BPC-157?
Not necessarily, because they target different aspects of tissue repair.
How long is a typical TB-500 loading phase?
Common protocols use a loading phase of about 4 to 6 weeks.
Should everyone stack TB-500 and BPC-157?
No, stacking depends on the injury, goals, budget, and personal preference rather than being universally necessary.
Resources:
Rahaman et al. (2024) — https://pubmed.ncbi.nlm.nih.gov/38382158/
Maar et al. (2025) — https://pubmed.ncbi.nlm.nih.gov/40362372/
Di et al. (2026) — https://pubmed.ncbi.nlm.nih.gov/41570941/
Zhu et al. (2016) — https://pubmed.ncbi.nlm.nih.gov/27288307/
Gao et al. (2015) — https://pubmed.ncbi.nlm.nih.gov/26083021/
Morris et al. (2018) — https://pmc.ncbi.nlm.nih.gov/articles/PMC6481613/
Kleinman and Sosne (2016) — https://www.sciencedirect.com/science/chapter/bookseries/abs/pii/S008367291630005X?via%3Dihub
Philp et al. (2003) — https://onlinelibrary.wiley.com/doi/10.1046/j.1524-475X.2003.11105.x
Xing et al. (2021) — https://pmc.ncbi.nlm.nih.gov/articles/PMC8724243/
SEER-1 Phase 3 Trial (2023) — https://pmc.ncbi.nlm.nih.gov/articles/PMC9820614/
ClinicalTrials.gov (NCT00832091) — https://clinicaltrials.gov/study/NCT00832091
Applied Sciences (2026) — https://www.mdpi.com/2076-3417/16/12/6202
He et al. (2022) — https://pmc.ncbi.nlm.nih.gov/articles/PMC9794587/
Lee and Burgess (2025) — https://pubmed.ncbi.nlm.nih.gov/40131143/
Mayfield et al. (2026) — https://pubmed.ncbi.nlm.nih.gov/41476424/
Jozwiak et al. (2025) — https://www.mdpi.com/1424-8247/18/2/185
Yuan et al. (2026) — https://www.mdpi.com/1422-0067/27/6/2876
FDA Federal Register (2026) — https://www.federalregister.gov/documents/2026/04/16/2026-07361/pharmacy-compounding-advisory-committee-notice-of-meeting-establishment-of-a-public-docket-request
WADA 2026 Prohibited List — https://www.wada-ama.org/en/resources/2026-prohibited-list
USADA — https://www.usada.org


